Chapter 8 of your book is generally good.
There are two different but related topics under "respiratory toxicology." First topic is inhaled toxicants that harm the respiratory tract, that is, the respiratory tract is the target organ. Second topic is toxicants that enter via the inhalation, but do their damage systemically. (There are a few chemicals that do the opposite, enter through via ingestion, then do their harm in the respiratory tract.
Here is a site to review, has better pictures: http://www.innerbody.com/anim/lungs.html
and the Tox Tudor section: https://training.seer.cancer.gov/anatomy/respiratory/
Big picture. The respiratory tract has to expose an enormous surface area to air across a very thin membrane in order to permit diffusion of oxygen into the blood and carbon dioxide to diffuse out of the blood. The surface area in an adult is about 800 square feet. The body provides this area by branching, from large conducting airways, a bronchus, that is stiffened with cartilage to prevent its collapse under suction, through constant branching into smaller and smaller bronchi, each branch having less cartilage, finally to the pulmonary region where gas transfer take place. As the bronchi get smaller and smaller, there are more of them and their surface area increases and cross sectional area increases, consequently the velocity of the gas gets smaller and smaller.
|
Name
|
X-sectional area
|
Velocity
|
Diameter, each
|
|
cm2
|
cm/sec
|
cm
|
|
|
Conducting Airways, with cartilage, cilia and mucus
|
|||
| (Major) Bronchus |
1.5
|
130
|
1.4
|
| Large Bronchi, typical |
3.1
|
65
|
0.2
|
| Small Bronchi, typical |
14
|
14
|
0.15
|
|
Conducting Airways, without cartilage, with smooth muscle,
cilia and mucus
|
|||
| Bronchioles |
150
|
1.3
|
0.06
|
| Terminal Bronchioles |
220
|
0.9
|
0.05
|
|
Pulmonary (gas transfer), surfactant
|
|||
| Respiratory bronchioles |
147,000
|
approx.. 0
|
0.03
|
| Alveoli, ducts and sacs |
750,000
|
0
|
|
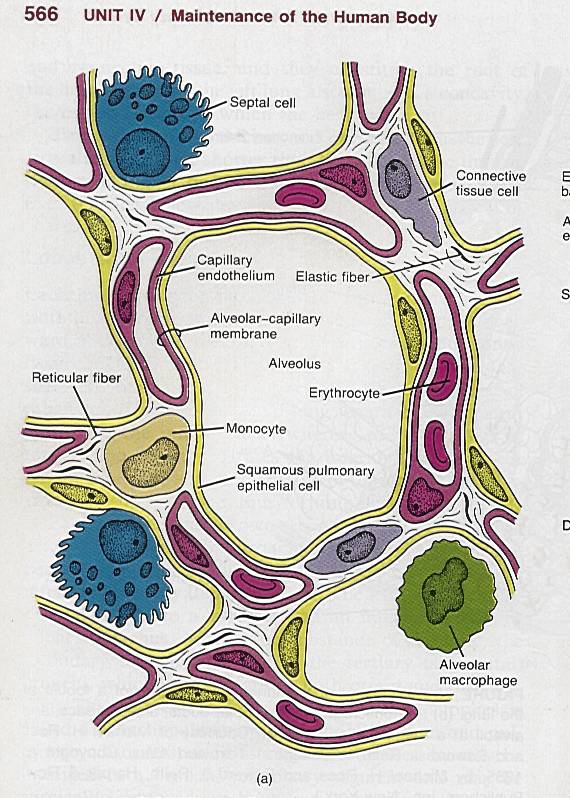
Here's a cartoon of a cross section through an alveolus. The yellow ring around the alveolus is a Type I pneumocyte (called a "squamous pulmonary epithelia cell" here). It is a cell with a thin wall. The "Septal cell" is now called a Type II pneumocyte, it is specialized to secrete surfactant, it actually makes up about 3% of the the surface of the alveoli, the other 97% of the surface is made of Type I cells. Surfactant is a soapy chemical that reduces the surface tension at the alveolar wall.
From Tortora and Anagnoskakos, Principles of Anatomy and Physiology, 5th ed, Copyright
The red rings are the capillaries. The doughnut shaped cells in the middle of those are red blood cells, called erythrocytes. The capillary is actually a tube made out of cells with very thin walls. The cells are called endothelial cells and the wall is the "endothelium." The alveolar-capillary membrane is very thin, typicality less than 0.5 um. It is here where gas is transferred. Two other cells types are shown, a monocyte is a type of white blood cell. The Alveolar macrophage is another type of white blood cell, it is not attached to the walls of the alveolus and moves around inside the alveolus. We'll talk more about macrophages in the submodule on asbestos. Some terminology: In most organs there is a "business end," the cellular portion of the organ that does the biochemical or mechanical function of the organ and this is called the parenchyma. The connective tissues that support these are called stroma. In the cartoon above, I'd call the Type I and II pneumocytes and the capillaries the "parenchyma" and the connective tissue the "stroma."
Absorption of chemicals along the respiratory tract (RT). Both the mucus on the conducting airways and the water and surfactant of pulmonary region are "watery." Hydrophilic chemicals are absorbed high in the RT. In addition, the nose has baffles (turbinates) designed to increase turbulence and thereby increase transfer of heat and mass in the nose. In rodents, who are obligatory nose breathers, most hydrophilic chemicals are absorbed there. Humans breath by both nose and mouth, so hydrophilic chemicals may make it further down the RT. In addition, the mucus is a glycoprotein, and reactive chemicals may bond to some chemical moiety in the mucus or diffuse into water. Many toxic gases are irritants to the upper respiratory tract (URT), formaldehyde is a reactive gas that irritates the URT. It is also a rodent carcinogen. Some chemicals, ethanol and methanol for example, are not reactive nor irritants but are absorbed in the URT. While the inhaled air is completely scrubbed of hydrophilic gas, on exhalation, the exhaled air, which is now clean, can absorb some of the gas back into the air stream. Hence absorption of hydrophilic gases is not 100%, 70% is a more likely number.
Hydrophobic chemicals are not well absorbed in the RT, but, in the alveoli there is an enormous surface area. The absorption of these chemicals is governed by the partitioning between the blood and the alveolar gas, and other parameters. One can estimate the amount of chemical absorbed by use of Physiologically-Based Pharmacokinetic Models (PBPK models). It turns out that the parameters can be quite different between laboratory rodents and humans, for example on a body weight basis, rodents breath 5 to 10 more than humans. PBPK models are used to estimate the blood concentrations in the different species and at different doses, in order to aid extrapolation between species.
End of Submodule